SAME OLD ways to fight a new virus
This paper was presented at the inaugural session of a webinar on the Covid-19 pandemic organised by MAC INSERCH on the occasion of World Environment Day on June 5, 2020. This blog has been edited for brevity.
Thank you for inviting me to this important Webinar that puts in perspective human health in relation to planet health. As we experience this historic pandemic of epic proportions, it is important for us to shift the focus away from ourselves and use the eye of the sharp eagle that swoops down on its prey hundreds of metres below, where it surveys all that lies beneath. If we do indeed adopt this approach, we will see the pandemic as a more holistic problem and thus explore solutions in areas that have perhaps not been pursued with as much vigour as let’s say – the search for a vaccine. But before we head in that direction, let us examine this problem.
Pandemics are not new. They have occurred frequently in human history, wiping out the weak and vulnerable, sometimes, even entire populations. Their scale, intensity and frequency has varied over time. A pandemic or even a widespread epidemic, does not just occur out of the blue. Typically, human interference with the environment builds up, causing a pandemic to reset the equation between humankind and nature. The plague of the 14th century, the most intense pandemic ever to have been recorded, killed 200 million people – nearly half the world’s population.
How did this occur? According to contemporary sources, climate change in Asia forced rodents out of drying grasslands to more populated areas, spreading the disease. It came from Central or East Asia to the Italian city of Genoa through the fabled Silk Road. It then travelled on merchant ships spreading throughout the Mediterranean Basin and reaching Africa, West Asia, and the rest of Europe via Constantinople, Sicily, and the Italian Peninsula. Current evidence indicates that once it came onshore, the Black Death was in large part spread by human fleas – which cause pneumonic plague – and the person-to-person contact via aerosols which pneumonic plague enables, thus explaining the very fast inland spread of the epidemic, which was faster than would be expected if the primary vector was rat fleas causing bubonic plague.
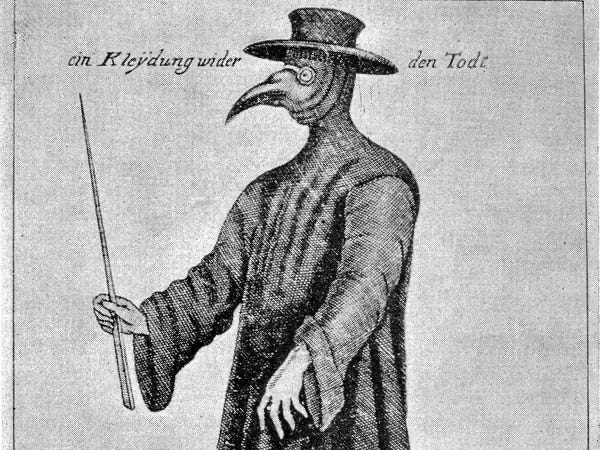
Dramatically called Black Death, because it claimed so many lives, this period also witnessed improvements in communication, increased trade, large-scale urbanisation and clearing vast tracts of forests for agricultural use. It also prompted medical research around diseases and their vectors and even though it was the medieval age, the practice of isolation, quarantining, hand washing to avoid and manage diseases became commonplace. This did not mean that the world would be rid of plague – it took a few more centuries of outbreaks and it was not until the early 20th century that any victory could be claimed. The plague of the 17th century was equally dramatic. During this time, we see first evidence of physicians adopting an early version of the PPE: a robe with a beak-like mask, gloves, and a long staff to keep distance while examining patients. The best way to protect people from the plague remained the same: hand washing, physical distance, isolation. Improved sanitation over time contributed immensely to reduce the frequency and intensity of outbreaks.
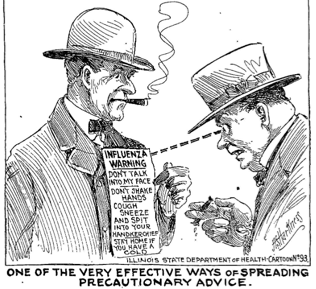
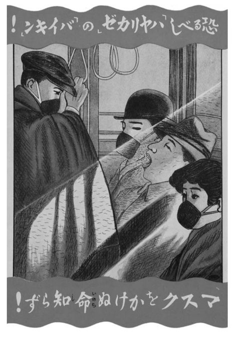
The flu epidemic that occurred a century ago was mysterious in both its origin – where and how it occurred; as well as its eventual disappearance. It is incorrectly referred as the Spanish Flu, but it spread all over the world, which was recovering from the First World War at the same time. As physicians and scientists, now equipped with more knowledge and even vaccines, grappled with casualties from the epidemic, the message to people was the same: stay away from the sick, keep them isolated, and wash your hands. This message was consistent from the US to Japan. Japanese communication material even depicts sneeziquette and the use of face masks in public places. Polio, a disease on the brink of eradication, also hinges on sustaining good hygiene and sanitation practices in addition to immunisation for stopping transmission. Almost every childhood and adult illness – diarrhoea, common cold, seasonal influenza – can be prevented by hand washing.
We can conclude that the methods of avoiding disease have remained consistent from the medieval age until now. Hand washing and physical distancing – whether this is interpreted as a one or two metre distance, isolation, quarantining – are still the best ways to keep ourselves safe.
Interestingly, communication material on Avian Influenza and H1N1 or the Swine Flu also stresses the importance of hand washing and physical distancing. It is almost as if the underlying message were: when in doubt, wash your hands!
So what is new about this pandemic? The virus, for one. The novel coronavirus COVID-19 is a new virus. It is just a few months old and has still not infected enough people to generate a body of verifiable knowledge. It is circulating in a world that is deeply interconnected and globalised and thus interdependent, and a world that has not previously supported a population of almost 8 billion. The world has been urbanised and exploited for its wealth and resources and the use of fossil fuels has still not diminished despite advancements in renewable energy. And despite having experienced relative peace for over seven decades, there are vast disparities of income and wealth. This exacerbates the pandemic, as not all nations can fight it equally. Here lies the simplicity of fighting the virus using old, tried and tested ways. So, the same messages of hand washing and physical distancing have become more specific. Let’s take hand washing. The message to wash your hands frequently comes with visuals on how to wash them properly. And just to make sure all the germs are washed, depending on the culture you belong to, you sing either the first verse of Happy Birthday or the National Anthem!
Similarly, the message around physical distancing, where I include recommendations to isolate or quarantine, have become more precise. There is ample historic evidence that these practices are not new. Many trade caravans spent their time in caravansarais outside city limits before being permitted to enter/re-enter. Caste Hindus lost their caste if they travelled abroad so as to discourage youth to return with illnesses. Common wisdom was that isolation for a period of time helped break chains of transmission. This behaviour is being widely recommended and reinforced. Depending on where you are, you stay anywhere between one and two metres away from other people in public places. There are now limits on how many people can gather in public while keeping this distance, so long as the virus circulates. In the event of a case in your building, all residents are under quarantine. In the event of a case in the family, there is the stricter protocol of isolation. But more importantly, the message to call the doctor for advice rather than visit and thus crowd the hospital or clinics is an example of how the distancing message has been nuanced.
The last message of calling and not visiting the doctor is also prompted by the fact that COVID-19 tends to disproportionately infect the old and those with underlying conditions or co-morbidities. It also affects caregivers and thus eats away at the healthcare resources of trained personnel who can provide intensive care. A majority of people who are infected by the virus are either asymptomatic or have very mild symptoms. We can discuss this separately as it does not directly relate to the main theme of my topic on how we are using the same old messages to fight a new virus.
There is one prevention message that is new. Since COVID-19 infection is marked by a distinct dry cough, it is recommended that we now practice cough etiquette and cover our mouth with elbows while coughing. Many cultures advise the use of masks although WHO has not advocated their use. Shaking hands, kissing and other forms of physical contact have been discouraged and can be treated under the broader category of distancing.
Are lockdowns new? This is an extension of the measure to physically distance yourself and distance yourself socially as well. The answer to this question, again, is no. The first record of a lockdown as part of an organised response to a health emergency was during the plague outbreak in Italy during the Renaissance[1]. More recently[2], although the spate of lockdowns was inspired by the lockdown of Hubei province in China when cases went out of control. There is recent memory of lockdowns during the Ebola outbreak in West Africa. However, these lockdowns in Sierra Leone and Liberia were preceded by intense microplanning and provisions of medical supplies and rations for communities that would be most vulnerable. The current scale of lockdown however, has not been seen before. We can discuss whether these have impact on stopping transmission – the short answer is that they work if (a) they are not extensive or indefinite, (b) there is complete transparency between the government and citizens; and (c) the channels of communication (media) are free and independent.
Lockdowns have forced families to live together under the same roof for prolonged periods exposing vulnerabilities of women and children, forcing us to redefine what constitutes a safe space. Domestic violence has doubled in almost every country where data is available, irrespective of whether they belong to the global north or south. Children are at greatest risk of cyber bullying, sexual exploitation, trafficking, violence and abuse. Since transport and movement is restricted, women and children remain imprisoned by their tormentors. Uber offered free rides and meals to women escaping domestic violence in 16 countries but has since laid off staff and drivers, so we don’t know if this will make an impact. But we do know that there is currently no escape and given that lockdowns are being extended, so will the trauma. Interestingly, and perhaps not surprisingly, even this feature (DV) has parallels with the plague pandemic of the 14th and 17th centuries where there are records of an increase in violence against women during the period. Subsequently, following the plague, many women were burnt alive as witches. Climate change contributed to this back then as well, as the earth started cooling and cropping patterns changed and food became scarce. What this parallel illustrates is the exacerbation of vulnerabilities in the event of uncertainty. Violence against women and children escalates when futures are not secure. Job losses as a result of this pandemic have also contributed to increased domestic violence.
Finally, given that we are dealing with this new virus using old methods, and given that we still don’t know enough about it, we are seeing a profusion of misinformation, finger-pointing, and conspiracy theories. Even this is not new. Jews were blamed for the plague. Today, we blame other groups – the Chinese for starting it, Muslim groups for propagating it. There are rumours around how the virus was created in a lab. It is important to recognise this misinformation for what it is and fight the myths and rumours. Governments and media play a very important part in combating misinformation by taking citizens into confidence, communicating clearly and frequently and being transparent.
Is nothing new? The global community as it exists since 1919 in a spirit of cooperation, collaboration, but above all, committed to protecting human rights, is a century old[3]. We therefore now have institutions like the UN and specialised agencies such as WHO and UNICEF that have led health and immunisation campaigns. We are so medically and scientifically advanced that the deaths from this pandemic are still lower than those from Ebola, for which, a vaccine was developed in record time. We have eradicated small pox and polio (almost) that once caused epidemics killing and crippling thousands, including FDR. Closer home, most of us live in countries that are committed to welfarism but have not made enough investments in strengthening public health systems and social protection mechanisms. There are facilities to enhance these investments and that of course, is new. Our awareness of social inequity has been enhanced through this pandemic as we see visuals of informal workers traversing the subcontinent for a safe haven as there is no provision for them when factories lock down indefinitely. Although this sounds absurd, mass migration unleashed by pandemics is again, not new. However, we will need to rebuild differently and more creatively. The response and recovery from this pandemic should be addressed in an inclusive and intersectoral manner, with many lessons from history. In particular, with an emphasis on mental well-being. In addition to the trauma of isolation, the trauma of abuse, domestic violence, child sexual abuse, loss of economic security draws attention to investing in mental health as a comprehensive part of a public health package.
While the plague of the 14th century and the flu epidemic of the previous century came without warning, those working on public health and many world leaders knew of the inevitability of a pandemic in our day. Yet, despite this privileged knowledge, we were all caught unprepared. Perhaps this unpreparedness resulted in the scale of lockdowns and reduction of economic activity we have witnessed. In highly industrialised countries, the reduction of carbon emissions resulted in blue skies that were plain to see. In the city of Delhi, notorious for its air pollution, face masks once used to protect against toxic air were ironically mandated to protect against the virus. Daily global carbon dioxide emissions were down by 17% according to a study by Le Quéré et al.[4] This is likely to climb back up quite rapidly as lockdowns lift, but if some of the measures are sustained until the end of 2020, these gains can be significant. Environmental healing after a pandemic is not new either – Black Death was followed by an age of cooling or a Little Ice Age that lasted nearly 500 years. We can only hope that we are part of the healing as Earth will always survive. Humans may yet write their destiny.
[1] Prof John Henderson in Florence Under Siege, Surviving Plague in an Early Modern City (Yale: 2019) discusses public health measures undertaken during the plague outbreak of the 17th Century in Italy to have influenced health policies today. These include the process of contact tracing and finding patient zero which was first undertaken in Florence. Authorities tried to identify the first person who brought the plague into the city or state and tracked down all their contacts who were then confined for forty days either in their homes or isolation centres outside the city. There was a considerable amount of vigilance by health authorities to ensure that people stayed home during the lockdown. People were however, allowed to stand on their balconies and communicate and sing – this was a feature of many European cities that faced lockdown during the covid-19 outbreak. It was during this time that cordons sanitaires were set up along state borders to stop people from travelling and thus carrying the plague.
[2] Ramin Jehanbegloo notes that lockdowns have also been prompted due to nuclear disasters such as Chernobyl and Fukushima as well as due to acts of terror such as 9/11. See also, https://www.livemint.com/news/india/life-lessons-from-the-history-of-lockdowns-11585312953744.html
[3] I include efforts at forging multilateral institutions for peace such as the League of Nations, which was a precursor to the United Nations.
[4] Le Quéré, C., Jackson, R.B., Jones, M.W. et al. Temporary reduction in daily global CO2 emissions during the COVID-19 forced confinement. Nat. Clim. Chang. (2020).

The writer, and the other stuff.
Hello. I’m Gitanjali — development practitioner, sometime author, full-time mother, and very part-time golfer. I’ve spent the last two decades working across South Asia, West Africa, and bits of the world in between, mostly on polio eradication, regional integration, global health, and gender.
This site is a collection of essays I started writing during the pandemic and never quite stopped. Some are field notes. Some are rants. Some are about the strange things you notice on a video call when you’re on your thousandth one. They are written from Switzerland, where I now live with my husband and our daughter.
Writing is how I figure out what I actually think. I publish in case any of it is useful — or, at minimum, mildly entertaining — to you.
If you’d like to get in touch, you can find me through the usual channels. Otherwise, thank you for reading.
Gitanjali
The writer, and the other stuff. Hello. I'm Gitanjali — development practitioner, sometime author, full-time mother, and very part-time golfer. I've spent the last two decades working across South Asia, West Africa, and bits of the world in between, mostly on polio eradication, regional integration, global health, and gender. This site is a collection of essays I started writing during the pandemic and never quite stopped. Some are field notes. Some are rants. Some are about the strange things you notice on a video call when you're on your thousandth one. They are written from Switzerland, where I now live with my husband and our daughter.
Writing is how I figure out what I actually think. I publish in case any of it is useful — or, at minimum, mildly entertaining — to you.If you'd like to get in touch, you can find me through the usual channels. Otherwise, thank you for reading.
One Comment
Pingback: